Wrongly Maligned
Wrongly Maligned
Cholesterol has been wrongly given a bad name. In fact, it is one of the truly essential building blocks of nature and we use it for such vital processes as making all of our hormones, repairing our tissues, producing bile from the liver etc.
Contrary to popular belief, cholesterol does not cause heart attacks, nor does it 'clog the arteries'. Heart attacks are caused by blood clots that are caused by damage to the lining of our blood vessels (the endothelium) and this, in turn, happens from diverse causes including excess inflammation, aging, physical trauma etc.
Keeping well hydrated, eating plenty of healthy and whole foods (which includes foods rich in fats) keeping active and keeping your liver healthy will do far more to prevent heart disease than taking statin drugs.
For example, comprehensive studies show that exercising regularly can increase life span for 4 and a half years whilst taking statin drugs for 5 years will give the average person an extra 4 days of life!
Conversely, statins are associated with many side effects, including fatigue, memory loss, insomnia, polymyalgia rheumatica, erectile dysfunction, neuropathy, diabetes, cataracts, kidney disease and loss of muscle strength.
Statistical analysis shows that the two times the benefits of statins may be worth the risk of side effects is when 1) people are already highly blocked in their arteries or 2) people who have just had a stroke or heart attack and had stents put in.
'The idea that saturated fats cause heart disease is completely wrong, but the statement has been published so many times over the last few decades that it is very difficult to convince people otherwise unless they are willing to take the time to read and learn what produced the anti-saturated fat agenda' Dr Mary Enig, consulting editor to the American College of Nutrition.
I have copied some of the research on cholesterol below, or to watch a 12 minute video that shows how the cholesterol myth started with shonky science, put this link in your browser
https://drmalcolmkendrick.org/statin-nation-the-documentary/
Cholesterol testing
Even if it is not anywhere near as bad for you as is made out, too much, or too little cholesterol can still be an important indicator that things may be out of balance and we frequently test our patients with an authorised medical device that gives a print-out of the person's lipid panel within a few minutes of testing.
The results of these tests often have me talking with my patients about increasing healthy fats in their diets because their levels of cholesterol are lower than they could be optimally!
When they are what is seen as dangerously above the normal range, most people don't realise that over 80% of their cholesterol is made in their liver and less than 20% of it comes from their diet. The main two reasons our livers make too much cholesterol are excess stress and a diet that is too high in carbohydrates
Excess Stress
We produce hormones when we are under excess stress that are largely made from cholesterol. Consequently, the more stress a person has the more stress hormones, and therefore cholesterol, they need to make. Stress is obviously a big subject in itself. Several articles on this site go into it in more depth, for example the sections on insomnia here, anxiety here, high blood pressure here, fatigue here, & depression here

Excess carbohydrates
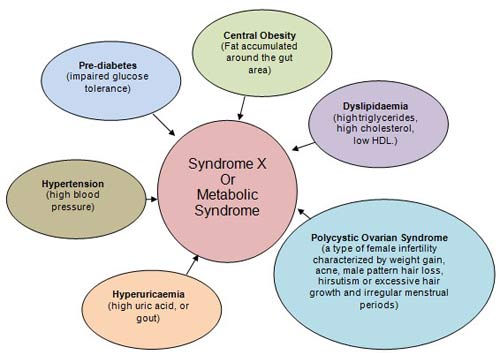
For many people, the root cause of their bad cholesterol is that they have the metabolic syndrome and so convert the excess sugars in their diet into fats. This important subject is discussed in detail in its own article here
 TOP | CONDITIONS TREATED A-Z or BY GROUP
TOP | CONDITIONS TREATED A-Z or BY GROUP
Herbal medicine for cholesterol.
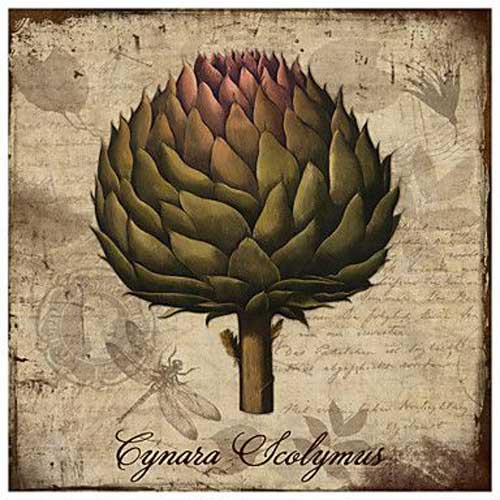
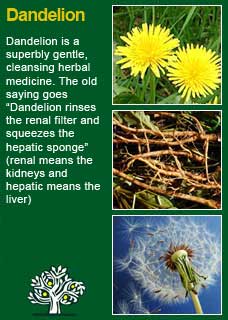
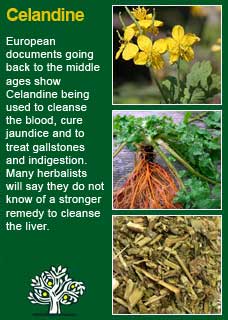
Caring for the liver with herbs such as Celandine, Barberry, Dandelion Root, Globe artichoke & Milk thistle has frequently seen excellent results for bad cholesterol readings. You can learn more about any of these key liver herbs in the A-Z here or in the article on liver health found here. It has also been of proven benefit to help reduce excess cholesterol and for losing weight to take Psyllium husks before food, more about them here

Cynara scolymus (Globe artichoke)
TOP | CONDITIONS TREATED A-Z or BY GROUP
Constitutional Health Note:
You might benefit from learning about your constitution to know what kind of foods and herbs will work especially well for you as well as many other interesting matters. Constitutional health is an old and fascinating way of understanding our differences and to demonstrate how it works in this area if you are a dryer constitution then you are rather less likely to have any issues with cholesterol to start with but for the damper constitutions the reverse is true, especially for the hotter and damper constitutions, the Tigers, who are clearly the most prone of the different constitutions to high cholesterol.
There is a brief introduction to this subject here and a more detailed section on working out which constitution you are here
TOP | CONDITIONS TREATED A-Z or BY GROUP
Articles on cholesterol
Here are several published articles on cholesterol and drug therapies that have a different view to the mainstream advice from conventional medicine. The articles are summarised below and then the full text is copied further down the page.
Combined Impact of Health Behaviours and Mortality in Men and Women
This study shows how some healthy behaviours (not smoking, eating fruit and vegies, being active and keeping alcohol moderate) could increase average life-span by 14 years
Reading the evidence closely — statins for seniors
The second article, copied below the first, shows on the other hand how taking statin drugs to lower cholesterol can increase average life span by 15 days (so long as the drugs are taken every day for 30 years!). This article is very detailed and I know it will be too much information for some but this whole area is so fraught with misinformation that I thought it would be a good one for people who really want to sink their teeth into some statistics!
Do statins save lives in essentially healthy people?
Lastly the article at the bottom of the page is by Dr John Briffa from 2010. It shows some alarming statistics including that more people are likely to get adverse side effects from statins than benefits from them! He finishes this article by saying "I’m not against statins (though I would not take them myself). What I am against, however, is individuals given one-sided or misleading information about their risks and benefits. I’ve found in practice that once individuals are given a more complete picture about the effects of these drugs, the vast majority of people are happy not to take them."

Combined Impact of Health Behaviours and Mortality in Men and Women:
The EPIC-Norfolk Prospective Population Study Published in PLOS medicine January 8 2008
Background
There is overwhelming evidence that behavioural factors influence health, but their combined impact on the general population is less well documented. We aimed to quantify the potential combined impact of four health behaviours on mortality in men and women living in the general community.
Methods and Findings
We examined the prospective relationship between lifestyle and mortality in a prospective population study of 20,244 men and women aged 45–79 y with no known cardiovascular disease or cancer at baseline survey in 1993–1997, living in the general community in the United Kingdom, and followed up to 2006. Participants scored one point for each health behaviour: current non-smoking, not physically inactive, moderate alcohol intake (1–14 units a week) and plasma vitamin C >50 mmol/l indicating fruit and vegetable intake of at least five servings a day, for a total score ranging from zero to four. After an average 11 y follow-up, the age-, sex-, body mass–, and social class–adjusted relative risks (95% confidence intervals) for all-cause mortality(1,987 deaths) for men and women who had three, two, one, and zero compared to four health behaviours were respectively, 1.39 (1.21–1.60), 1.95 (1.70–-2.25), 2.52 (2.13–3.00), and 4.04 (2.95–5.54) p < 0.001 trend. The relationships were consistent in subgroups stratified by sex, age, body mass index, and social class, and after excluding deaths within 2 y. The trends were strongest for cardiovascular causes. The mortality risk for those with four compared to zero health behaviours was equivalent to being 14 years younger in chronological age.
Conclusions
Four health behaviours combined predict a 4-fold difference in total mortality in men and women, with an estimated impact equivalent to 14 years in chronological age.
Citation: Khaw K-T, Wareham N, Bingham S, Welch A, Luben R, et al. (2008) Combined Impact of Health Behaviours and Mortality in Men and Women: The EPIC-Norfolk Prospective Population Study. PLoS Med 5(1): e12. doi:10.1371/journal.pmed.0050012
Academic Editor: Alan Lopez, The University of Queensland, Australia
Received: July 18, 2007; Accepted: October 26, 2007; Published: January 8, 2008
Copyright: 2008 Khaw et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Funding: EPIC-Norfolk is supported by programme grants from Medical Research Council and Cancer Research United Kingdom with additional support from the Stroke Association, British Heart Foundation, Research Into Ageing, and the Academy of Medical Science. The sponsors had no role in the design and conduct of the study, collection, management, analysis and interpretation of the data, and preparation, review, or approval of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
Abbreviations: CI, confidence interval; ICD, International Classification of Disease; RR, relative risk

Taraxacum officinale (Dandelion)
TOP | CONDITIONS TREATED A-Z or BY GROUP
Reading the evidence closely — statins for seniors
Recent news has reported that new research offers evidence for the benefits of taking statins for the elderly and for women — two groups of people in which statins have been especially controversial and not widely prescribed. Today, we’ll look at this new study on the use of statins in seniors.
To help us make the soundest health decisions for ourselves or a loved one, it’s first crucial to understand how clinical studies are reported. Oftentimes, the way results are reported don’t mean what we think they do.
And the mainstream media rarely gives the types of in-depth analyses of studies and the full information for us to be able to make informed decisions. Most of the news presents statins as if the science is settled and incontrovertible (there’s no need to repeat those stories here). So, many people may be surprised to learn of the medical debates that don’t regularly make the news.
Understanding risks — relative versus absolute
The largest body of evidence behind the use of statins has come from studies done on middle-aged men, rather than seniors or women. An editorial in today’s British Medical Journal gave a timely and helpful look at the difficulties for doctors and patients in sorting out the benefits and risks for statins, even for this most widely prescribed group of people. Dr. Des Spence from Glasgow wrote:
Whether it’s worth treating high cholesterol is a common enough question. No one who sees the charts and listens to the sales pitch [and media] would doubt it — but numbers are open to being spun. Let’s consider the trial known as WOSCOPS... The participants were men aged between 45 and 64 in the most socially deprived area in Western Europe. More than three quarters (78%) were current or former smokers, and their average cholesterol concentration was 7 mmol/l [271 mg/dl]. If lowering of cholesterol concentration was going to work anywhere it was going to work here. The study ran for five years, and the researchers reported a 32% reduction in cardiovascular mortality in the group of men who took statins....
But, this impressive-sounding figure is a relative risk reduction, not the reduction seen in actual (absolute) heart disease deaths. So a woman might, for instance, lower her actual risk of dying from heart disease from 0.5% to 0.34% — by a mere 0.16% — not nearly as impressive as 32%!
The real (absolute) numbers are important to know.
Dr. Spence went on to explain that for the men in the WOSCOPS trial:
Converting the 32% relative risk reduction into an absolute reduction gives a derisory 0.7% reduction in cardiovascular mortality and a number needed to treat of 143 over the study period.... So, putting it crudely, some 714 patients a year gain no benefit from treatment, even in the highest risk population in the world.... This is the “treatment paradox": that an individual patient, despite many years of investment in taking statins, gets virtually nil health benefit. Any relative benefit is seen only at the population level, even for composite cardiovascular endpoints. The treatment paradox is true of all treatable risk factors such as hypertension and osteoporosis.
Dr. Malcolm Kendrick, author of The Great Cholesterol Con, put these numbers into an even more meaningful perspective for an individual man. First, he cautioned that it’s easy to misinterpret that “numbers needed to treat” figure as suggesting a cure. “Statins do not treat/cure death, they only delay it,” he wrote.
Assuming that you do gain one entire extra year of life for every 700 years of taking a statin, he explained, this means:
[I]f you treated someone for 30 years you can expect to provide them with 30/700 added years of life. This is 15.64 days... In short, if a fifty year old man asked you how much longer he could expect to live if he took a statin for thirty years you can inform him “just over two weeks — max.”
The rationale for treating elderly people with statins, however, is even “less clear because the association between plasma cholesterol and risk of coronary artery disease diminishes with increasing age,” said Dr. James Shepherd, M.D. and colleagues at the University of Glasgow, Royal Infirmary, Scotland. In fact, they said, “in the oldest old people, low plasma cholesterol is associated with increased mortality.” This has been recognized in the medical literature, they said, (examples here, here and here) for some two decades, while not widely known among the public.
This seeming paradox led these researchers to conduct the largest ever randomized controlled clinical trial of statin use in older seniors, at the greatest risk for dying and developing cardiovascular disease and strokes. The PROspective Study of Pravastatin in the Elderly at Risk (PROSPER) trial randomized 5,804 seniors, 70-82 years old, to a pravastatin (statin) or placebo group and followed them for 3.2 years. The results were published in a 2002 issue of Lancet. The study was popularly reported as supporting a benefit of statins in reducing coronary heart disease-related deaths for the elderly and the results reported in terms of a 24% reduction in relative risk. The actual rates of heart disease deaths, however, were 3.3% among the group on statins, compared to 4.2% among the placebo group — an actual (absolute) difference of only 0.9%.
Yet even this absolute risk was not the full story. This is only one of several wordsmithing things to pay close attention to when we read about the results of a study, so that we can understand what is being reported and what it means for us.
Meaningful endpoints
The endpoint that people most care about is whether the treatment actually prolongs life, which makes total mortality the most important consideration, not just heart disease mortality. The PROSPER trial found that while there were slightly fewer deaths from heart disease, there were more deaths from other causes, such as cancers and strokes. The all-cause mortality in this study differed by only 0.2% (10.3% in statin group and 10.5% in placebo control group). This is a clinically insignificant difference, and led three dozen professionals to write the National Institutes of Health to raise serious concerns about the lack of scientific evidence behind recommendations for statin use in elderly patients.
When you read statin studies, more commonly their benefits are described as reducing risks for surrogate endpoints, such as lab values, or for nonfatal cardiovascular events and unstable angina, and all-cause mortality isn’t mentioned at all.
Compounding the difficulty of determining if statins benefit the elderly has been the limited number of studies on them. Prior to the publication of the PROSPER trial in 2002, Dr. Scott Grundy, M.D. wrote aneditorial for Archives of Internal Medicine saying: “To date, published clinical trials of statin therapy have not specifically targeted older persons... Without question, the lack of clinical trials that were designed specifically to test efficacy in older persons has been one factor standing in the way of a more forceful recommendation for intensive cholesterol-lowering therapy in this age group.” He argued for statin use in seniors 65 to 75 years of age, however, based on a subgroup analysis of seniors among the participants in other large trials which “strongly suggests that statin therapy significantly reduces risk in the age group.”
Dr. Uffe Ravnskov, M.D., Ph.D., a cholesterol researcher from Lund, Sweden, and colleagues, disagreed. As they explained, rather than relative risks, a more “honest way to inform the patient is to calculate his/her chance of surviving with and without treatment.” The personal odds for someone to benefit from any preventive drug or treatment is what people care about most: “What’s in it for me?”
They examined the actual chances of surviving, along with the relative risks and the absolute (actual) change in mortality, in the five trials Dr. Grundy used, as well as the large EXCEL (Expanded Clinical Evaluation of Lovastatin) double-blind, diet- and placebo-controlled trial of 8,245 seniors that he’d not included. They found that “the optimistic figures for relative risk reduction actually reflect unimpressive absolute risk reductions. These small benefits are also illustrated by the trivial differences between the survival rates with and without treatment.”
They compiled one of the clearest illustrations of the importance of looking at actual risks in order to gain a better understanding of what study findings mean:
They went on to examine other issues of statin use in elderly, such as mode of action and dosage. But they also highlighted yet another clinical consideration for anyone trying to weigh the risks and benefits of any medication. Just looking at mortality figures during a study period doesn’t consider potentially serious long-term side effects of statins, such as statin-induced myopathy, which is more frequent among the elderly, as Dr. Grundy cautioned. With advancing age, risk-benefits differ considerably from younger people and elderly are often more susceptible to adverse reactions. Drug metabolism is reduced in them and they are more likely to be on multiple drugs, to have multi-system conditions and to be underweight. According to Dr. Ravnskov and colleagues:
One may question whether statin treatment should be used at all because the small absolute risk reduction rewards may be outweighed by potential serious long-term side effects.
Whatever viewpoint you take away from the evidence, what is clear is that there appears considerable debate even among experts and each individual's decision may be different.
The latest evidence for statins in elderly
This past week brought news of a study purported to show statins, as a secondary prevention, reduce all-cause mortality in elderly heart disease patients. Researchers, led by Dr. Jonathan Afilalo, M.D., with McGill University in Montreal, Canada, published the results of their meta-analysis in the Journal of the American College of Cardiology.
Their working premise was: “Statins continue to be underutilized in elderly patients because evidence has not consistently shown that they reduce mortality.”
The authors searched through five electronic databases for trials published since 1966 that had examined statins use and included at least 50 elderly patients with documented cardiovascular disease. They identified 729 studies and winnowed them down, based on their inclusion criteria, to nine papers. The data in five studies they selected, however, had never been published and they did not obtain individual patient data from the authors, but extracted overall study data. Their inclusion criteria required each study to have data on all five outcomes: all-cause mortality, CHD mortality, nonfatal MI, need for revascularization and strokes. But the studies all had multiple different working hypotheses, used differing statins and doses, and were designed to examine different endpoints. Statin use among the control groups also varied from 2% to 24%. Women represented very small percentages of the study populations in each of their papers, but they believed that gender was not a significant effect modifier.
The Canadian researchers then used Bayesian forest plots with posterior relative risk estimates modeling for each study and pooled the relative risk estimates for five year follow-up periods. The five unpublished papers they used, however, had only followed the patients for 9 months to 3.9 years!
Already, we’re seeing some of the problems with meta-analyses, as has been previously reviewed.The studies lumped together in a meta-analysis can vary considerably in quality, measures, populations, methodologies and statistical analyses. Some studies may show a weak positive finding, others report none, and others may even report a negative finding. Meta-analyses can end up giving the same weight to all the studies (well-conducted and bad) by pooling them together, trying to create a statistically stronger estimation of an effect or prove something the studies weren’t designed to test. And therein lies the rub.
The Canadian study concluded:
In elderly patients with documented CHD, statins reduce all-cause mortality by 22% ... These estimates are rigorous and precise, owing in large part to our Bayesian hierarchical model and larger sample size of elderly patients, who had historically been under-represented in clinical trials. Achieving a high level of precision was critical, because summary odds ratios for all-cause mortality from 23 meta-analyses had been variable and heterogeneous.
This 22% reduction in relative risk, however did not reach statistical significance. In fact, their estimated pooled differences in absolute 5-year, all-cause mortality between the statin and placebo groups differed by only 3.1%.
In contrast to other studies, their model also showed increasing benefits from statins with age, even though none of the trials used in their meta-analysis included people over the age of 82, and the average age among the study populations was 69 years. Nevertheless, they concluded:
One of the most interesting findings of this study was that older patients attained a greater reduction than younger patients; the relative risk reduction for all-cause mortality was 50% in patients aged 80 to 97, 44% in patients aged 65 to 79, and 30% in patients aged 65 years.
They went on to conclude that their meta-analysis supported their premise and the need for doctors to change their statin prescribing habits for elderly patients:
Our meta-analysis adds to the current body of literature by showing that statins reduce all-cause mortality in elderly patients and that the magnitude of this effect is substantially larger than previously estimated....However, recently reported [statin] utilization rates of 40% to 60% in elderly patients with active CHD remain suboptimal. It is crucial to disseminate the evidence for statins in elderly patients with CHD to increase current utilization rates.
As the conclusions of the Canadian authors overstate the evidence they reported, one might wonder what, if any, conflicts of interest might be inadvertently influencing their analysis. But this published study had no Disclosure Statement, which is highly unusual for published studies.
An accompanying editorial in that same issue of the Journal of the American College of Cardiology discussed the problems that “continue to plague statin therapy in clinical practice: long-term adherence remains poor; and the treatment gap, especially among the elderly, remains large.” Doctors George A. Diamond and Sanjay Kaul of the University of California, Los Angeles, opined that the Centers for Medicare and Medicaid should discount drug prices to incentivize increased usage for those statins that show greater benefits, just as private insurers are already beginning to do. “A high discount will not erode the manufacturer’s profits,” they said. “In fact, profits are more likely to soar as a result of facilitated access to the less-costly drug and favorable shifts in market share.”
They said that statins are an example of the disconnect between what providers should do, according to the evidence, and what they’re paid to do:
This situation will not change unless and until we realign the financial and scientific incentives and begin rewarding caregivers, not for the prodigal provision of products and services, but for the enlightened provision of therapeutic benefit. Evidence-based reimbursement can be the bridge to this “far, far better thing."
Dilemmas for patients and doctors
When trying to decide what might be best for us or an elderly loved one, irrefutable evidence or at least all of the facts are needed so that we can weigh the risks and benefits. Yet other crucial information was missing from this recent meta-analysis and not considered in its conclusions. The Canadian researchers did not pool adverse events “because of failure to report these events stratified by age group in most studies and inconsistencies in classification of these events between studies.” So, they didn’t conduct a safety analysis to determine if the benefits of statin use outweighed the possible adverse events seniors might experience.
As recently reviewed here, evidence from younger populations for preventive health care interventions cannot be extrapolated to the elderly. Seniors are at special risk for adverse effects.
One of the clearest examinations of the adverse side effects being reported among statin users and the implications for the care of elderly patients was written by Dr. Beatrice A. Golomb, M.D., Ph.D., with the University of California, San Diego. As she wrote in Geriatric Times:
[A]ll drugs have potential adverse reactions despite their potential benefits. Understanding these risks is vitally important, particularly in elderly patients in whom both risks and benefits differ relative to younger patients. Evidence suggests the balance of benefits to risks may be less favorable in the elderly: Cholesterol becomes a less potent predictor of cardiovascular problems, and adverse reactions from drugs, including statins, may become more prominent.
Her paper examined the most common statin adverse effects recorded in the University of California at San Diego Statin Study, including muscular problems, worsening cognitive function, gastrointestinal and neurological effects, psychiatric problems, immune effects (e.g., lupus-like syndrome), erectile dysfunction and gynecomastia (breast enlargement in men), rash and skin problems and sleep problems. She even cautioned against discarding the significance of higher incidences of cancers seen in the PROSPER trial of elderly patients based on the risks seen in studies of younger patients.
Making individual clinical decisions is never easy or as simple and one-size-fits-all as it can seem in the news. The low rates of statins being prescribed for elderly might not reflect doctors’ or patients’ lack of awareness of the evidence, as some have suggested, but a greater awareness. Perhaps doctors and patients have weighed the potential pluses and minuses and decided that, for them, statins were not best.
Will that choice continue to be an option, or will statins become mandated performance measures for doctors, as already seen in some places, and obligatory for patients in order to receive medical care without being labeled as “noncompliant?” The importance of the best evidence behind clinical care guidelines impacts healthcare in ways many people might never imagine. One reader shared the difficulties she was having in finding a doctor to care for unrelated health problems because of, she believes, her decision not to take statins. As she told JFS: “No physician is obliged by law to take me if I won’t comply with 'standard of care.' I must take statins or I have no doctor.
Published in J Science 2008

Chelidonium majus (Celandine)
TOP | CONDITIONS TREATED A-Z or BY GROUP
Do statins save lives in essentially healthy people?
By Dr John Briffa on 30 June 2010 in Cholesterol and Statins, Food and Medical Politics
Statins are drugs that reduce cholesterol. They also reduce risk of heart disease and stroke. That does not mean, though, that they do this via their cholesterol-reducing effect. There are several lines of evidence which actually suggest otherwise. For example, statins can have clinical benefit before they reduce cholesterol levels. They also have been purported to reduce risk of heart events (like heart attack) in individuals who have ‘normal’ (non-elevated) cholesterol. And then we have the fact that cholesterol reduction through other means (other drugs, diet) has been shown to have no broad benefits for health (see here and here for more about this).
The fact the statins are unlikely to ‘work’ due their cholesterol-reducing effects is not a reason not to take then, however. It is a reason, however, to perhaps take the focus off cholesterol-reduction and put it on things that work better. And, of course even if statins do reduce the risk of cardiovascular disease, it at least makes sense to weigh up their risks and benefits over time.
A recent study in the British Medical Journal assessed the risks/benefits of statin therapy [1]. Here, in short, are the findings of this study:
For women, for every 10,000 high risk individuals treated with statins, there would be approximately 271 fewer cases of cardiovascular disease, 8 fewer cases of oesophageal cancer; 23 extra patients with acute renal [kidney] failure, 307 extra patients with cataracts; 74 extra patients who experience liver dysfunction; and 39 extra patients with myopathy [muscle pain and/or weakness].
For men, for every 10,000 high risk individuals treated with statins, there would be approximately 301 fewer cases of cardiovascular disease, 9 fewer cases of oesophageal cancer; 29 extra patients with acute renal failure, 191 extra patients with cataracts; 71 extra patients who experience liver dysfunction; and 110 extra patients with myopathy.
So, even in individuals at high risk of cardiovascular disease (i.e. those most likely to benefit from statin therapy), you have to treat lots of people with statins for one to benefit. But the reality is, more people will end up with a serious adverse effect as a result of treatment. Now, some would regard having a shot at preventing cardiovascular disease outweighs the other ‘less important’ risks. However, I suggest there are also those who would look at these statistics and reason that there really is little or no overall benefit to taking statins (and who could blame them). More about this later.
However, some will argue that it’s clear that statins benefits outweigh their harm on the basis that the reduce risk of death (overall mortality). Actually, there is an element of truth in this. However, it is important here to define better the sort of people who might take statins. Statin therapy broadly divides into two main approaches:
Primary prevention – where statins are given to essentially healthy people with no known cardiovascular disease (i.e. there is no evidence of arterial disease and no history of a heart attack and/or stroke)
Secondary prevention – where statins are given to people with known arterial disease and/or a history of heart attack and/or stroke
This distinction is important because individuals in the secondary prevention category are at generally high risk of further problems, and stand to benefit most from statin therapy. On the other hand, individuals in the primary prevention category are at generally low risk of cardiovascular disease issues (such as heart attack and stroke), and may therefore not benefit much from a strategy or treatment intended to prevent cardiovascular disease. This primary prevention category is particularly important when one considers that the vast majority of people taking statins are in this category, and if the pharmaceutical industry and some of its hired hands in the scientific and medical community have their way, increasing numbers of people will be taking statins in the future.
OK, back to the evidence…
There is indeed evidence that in secondary prevention, statins have the ability to save lives. One meta-analysis (lumping together of similar studies), for instance, found that in people with known heart disease, statin therapy reduced risk of death by 16 per cent [2].
But what about the more numerous primary prevention people? Do statins reduce risk of death in this population? That was the question asked by a study published this week in the Archives of Internal Medicine [3]. This study was a meta-analysis of 11 trials that included data on more than 65,000 people. An accompanying editorial [4] described this meta-analysis as “to date the cleanest and most complete meta-analysis of pharmacological lipid lowering for primary prevention.”
Cleanest, because the reviewed studies included primary prevention individuals only. The reason why this is important is highlighted by the authors in the following passage: “Limiting the analysis to patients without existing coronary disease is critical because studies that include both groups of patients may appear to show benefit for all patients, when all the benefit accrues to those with existing disease.”
This huge and relevant study showed that statin use is NOT associated with a reduced risk of mortality in the primary prevention setting.
The editorial also points out attention to the fact that in trials, individuals deemed to be at high risk of adverse effects, who take other medications and/or have other complicating illnesses are usually disallowed from taking part. However, this is not the case in the real world, where doctors commonly prescribe statins to more-or-less anyone with a raised cholesterol level (and increasingly, to people with normal cholesterol levels too). As a result, serious adverse effects may manifest that were not detected in the healthier trial subjects.
The editorial also highlights the fact that the trials are generally short (5-7 years), while use in the real world can go on for decades.
Some argue for statins on the basis that benefits are likely to accrue over time. But, this stance has no basis in science as, again, the editorial points out (we simply do not know one way or the other). The editorial authors also comment that the meta-analysis “…makes it clear that in the short term, for true primary prevention, the benefit, if any, is very small”.
I’m not against statins (though I would not take them myself). What I am against, however, is individuals given one-sided or misleading information about their risks and benefits. I’ve found in practice that once individuals are given a more complete picture about the effects of these drugs, the vast majority of people are happy not to take them.
References:
1. Hippisley-Cox J, et al. Unintended effects of statins in men and women in England and Wales: population based cohort study using the QResearch database BMJ 2010;340:c2197
2. Wilt TJ, et al. Effectiveness of statin therapy in adults with coronary heart disease. Arch Intern
Med 2004;164(13):1427-36
3. Ray KK, et al. Statins and all-cause mortality in high-risk primary prevention: a meta-analysis of 11 randomized controlled trials involving 65 229 participants. Arch Intern Med. 2010;170(12):1024-1031
4. Green LA. Cholesterol-Lowering Therapy for Primary Prevention – Still Much We Don’t Know. Arch Intern Med. 2010;170(12):1007-1008.
Dr John Briffa from 2010.